
The Endgame
Newsletter #58 - The kingdom of the sick (3)

Toronto, March 10, 2024
The kingdom of the sick (3)
My recent sojourn in the kingdom of the sick (see newsletters #56 and #57) got me thinking about Canadian Medicare. That lead me to this modest proposal which might encourage more discipline in the system and provide it with extra revenue. Apologies: I’m afraid the proposal is a bit nerdy.
The average Canadian thinks that medical care in Canada (most of it, at any rate) is free. After all, if you go to see the doctor, or get an x-ray, or have a blood test, you don’t have to put your hand in your pocket. But, of course, medical care in Canada is far from free. The 2023 national bill was about $350 billion, which is around $9,000 per Canadian and 13 per cent of GDP. This cost is met through general tax revenues. You pay plenty for medical treatment, just not at point of use.
The idea that medical care is free is pervasive. It’s often touted as one of the things that makes Canada special. But the idea is dangerous. It distorts the system. It promotes unnecessary use of medical resources, straining a system already under pressure. If medical treatment is free, well then, go for it. Why not? It’s human nature.
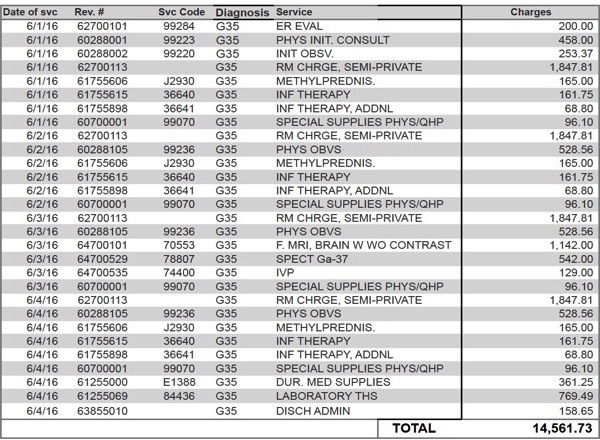
Once a year, at tax time, the government should send everyone a detailed statement of the cost of Medicare services they received in the previous taxation year. Wow, who knew that all those visits to the doctor cost so much in total? Maybe I don’t need to see her that often. I acknowledge there is a fine line to walk. Encouraging restraint in use of the health system should not be done in a way that discourages sensible preventative and early diagnosis measures. The modified system should be designed to take this into account.
Every Medicare participant should have an annual base entitlement to a specified dollar amount of services, let’s say $10,000. That means that the first $10,000 of services you receive in a given taxation year, as set out in your annual Medicare statement, attracts no additional payment obligation. If you consume less than this base entitlement, the difference is carried forward and is added to your base entitlement for the following year, and so on, i.e., you bank the difference. If you consume more than $10,000, the excess is added to your taxable income for the year. The advantage of taxing the excess as income is that’s it progressive, i.e., the cost to poorer people would be less than the cost to rich people. The tax revenue earned by taxing the excess would be earmarked for improvement and expansion of Medicare.
High earners might complain of double taxation under this proposal. For them, arguably, the modest base entitlement would be less than that portion of the income tax they already pay that could be considered their contribution to the cost of medical care. (The Fraser Institute estimates that in 2023 the 10 per cent of Canadian families with the lowest incomes paid an average of about $644 for public health care insurance. Families among the top 10 percent of income earners in Canada paid $44,314.) This double taxation argument should be rejected. A modified Medicare system that provides the same health entitlement for all Canadians would reflect the principle of equality that has always been the system’s backbone.
The annual base entitlement would have to be modified or waived for those with serious chronic conditions and those who face catastrophic illness. The cost of their care would greatly exceed the entitlement. In such cases, a Medicare Entitlement Board, upon application, could grant an exemption from the system, or adjust the base entitlement upwards as appropriate.
The Canadian Medicare system is brilliant. But it could be better. Less demand, more money.
An interesting comment on newsletter #57
A reader who used to live in Canada but now lives in France thought my swipe at the Canada Revenue Agency in #57 was unfair. He wrote: “My experience with the CRA, OAS, CPP, the Government of Canada in general has been a dream, and I have had a multitude of interactions with them since moving to France: polite, responsible (they always start by giving you their name and matricule. Try to get this from a French civil servant!), most helpful, kind, professional, calling you back in France several times when you leave a message.”
I've really enjoyed 'The Endgame.' Great writing, and interesting ideas, but...
I'd suggest staying in your lane. As a guy who has written about social policy for more than half a century, I am afraid that your ideas for 'saving' health care are old hat, have been discussed and tried and are wrong and/or impractical in both theory and practice.
First, you need to have a better understanding of health economics. Like some markets, health care is highly imperfect. Decisions on major expenditures are made by agents acting, supposedly, on behalf of the health care consumer, not by the consumer him or herself. You cannot walk into a hospital and decide to have a by-pass operation or a hip replacement. The decisions that are made by consumers are the least expensive parts of the system, such as whether to visit a primary physician, get a vaccine, go to an emergency room. All of these in themselves have negligible costs in the total system. Deterring these visits may even add to costs by delaying treatment.
One 'experiment' done in Canada when Ross Thatcher put user charges on patient-initiated services resulted in a decrease among person with low incomes and an increase among those with higher incomes for whom the charges meant nothing. I suppose the charges made people feel entitled. Also, doctors had to compensate for the income lost due to fewer visits by low income patients.
An actual experiment by the Rand Corp in the US found a deterrent effect among patients, but failed to look at the systemic effects overall (they only looked at the effects on the individuals paying a user fee).
As to deterring unhealthy behaviour, good luck with that! I suppose you can see how much lower obesity is in the US than Europe and Canada (NOT).
As to the idea of issuing a notice of the cost of services used, I recall that one province did try this (I'm too lazy to do any research and look it up). This added considerable costs to the overall system. Every doctor's office, lab, hospital, etc. had to hire people or extend hours and set up new systems. The verisimilitude of the accounts were proportional to the money spent on the system. How much should your account be for a one night in the general ward of the hospital? Should it be the marginal costs for the room (which would be very little) or the average costs (which would be a lot)? Should it be based retrospectively on last year's costs or prospectively on this years costs? More in the winter during flu season and less in the summer? Should it be a lot more for, say, the cardiac ICU?
In any case, as I recall, most people just throw out the invoice barely paying any attention to it since they did not have to do anything. But others had the bejesus scared out of them. Complaints and inquiries ensued. For what benefit? None, as far as anyone could assess.
Of course, if you are going to make the expenses taxable beyond a certain amount the bills had better be accurate, so get ready to expand spending on the health care system by a lot -- 10% or so like in the US perhaps? -- without adding any actual health care. What effect will these charges have? Tax the people who have been very sick? But people lucky enough not to have been sick pay nothing? Tell me this: if lack of revenue is the problem, why not just raise income tax rates on the wealthiest? This would entail no administrative costs at all, but presumably have the same economic costs as a health service related tax increase. Why is it fair to charge people in the time of the greatest need and not when they can better afford it? What exactly does this accomplish? Bottom line: if it is more tax revenue that is needed there are a lot simpler, fairer and less expensive ways to get it.
Anyway, I shall stop my rant here, encouraging you to continue the 'Endgame' to which I look forward each week.
I agree that we falsely claim our health system is free and that a yearly breakdown of services provided and received would be useful. Do we over or under use the system? Have the services been effective in resolving our ailment, would be another question to ask. I believe, based on personal experience and preference, that including services such as acupuncture, massage, osteopathy, along with many other such services, can more effectively and less expensively address and resolve certain common health conditions and complaints. Our narrow view of what constitutes health care is problematic and, therefore, the approach to resolving ailments is narrow. I rarely visit a medical doctor, but I can't afford the non-medical treatments that are labelled 'alternatives.' It is these alternatives, a few mentioned above, that have brought me more relief from physical injuries as well as overall improved well-being.